|
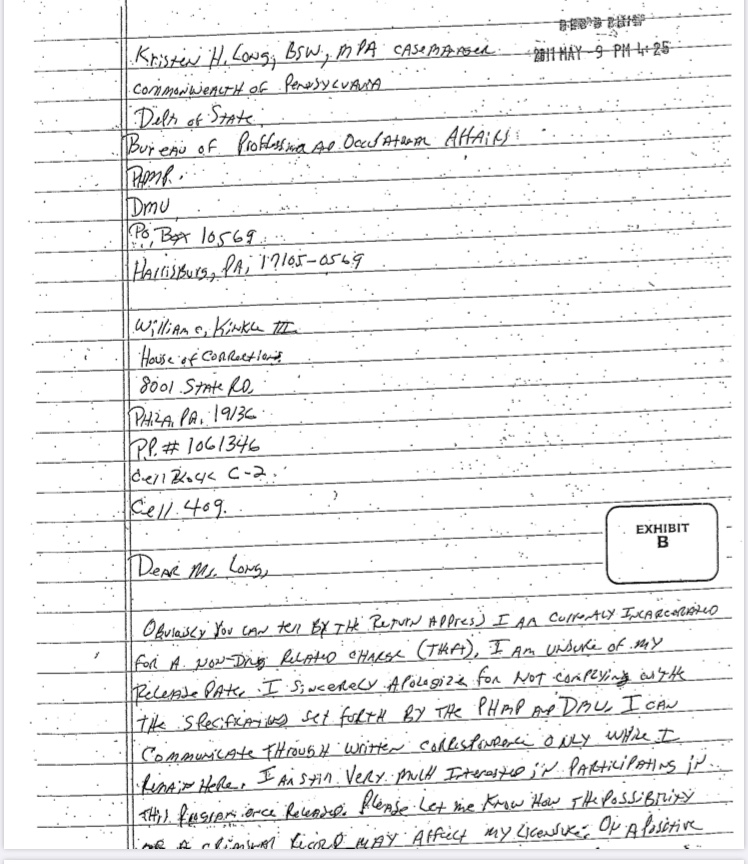
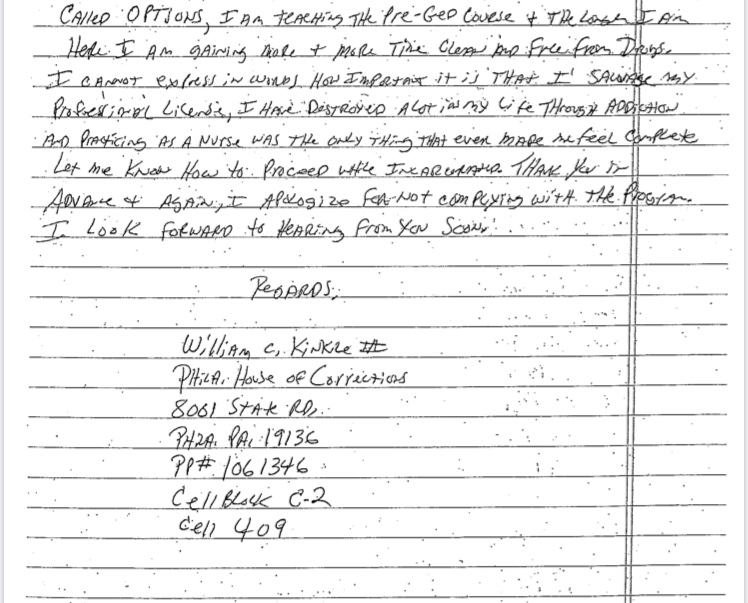
Many people have asked about the timeline of events that led to my nursing license being suspended. This post is to help clarify the details and highlight the discrimination with how we deal with healthcare professionals who suffer with substance use disorders. I began using opioids in 2008 to treat depression resulting from an abrupt divorce. Within 8 months or so after I started injecting heroin I lost everything, my job, housing etc. and was living on the street. During the first few months I was so ashamed and embarrassed I was reluctant to tell anyone, only 2 friends knew and they repeatedly told me to stay quiet in an effort to “protect my (nursing) license. I had also been working in emergency medicine for 15 years at that point and knew how we historically treated people suffering from addiction, so I said nothing. I took 2 FMLA leave of absences and after the second one I never returned to work. I was eventually fired. After about 14 months on the street I entered my first inpatient treatment center. This is where I was introduced to 12-step recovery. At this time I was an atheist in terms of spiritual beliefs and I could not grasp suffering with what was considered a medical illness, yet I was told the only way to get my disease into remission was through prayer, penitence, forgiveness and a spiritual awakening. I was administratively discharged (the clinical term for being kicked out) of this rehab (Cirque Lodge in Provo, Utah) for refusing to believe in god and participating in group prayer. I had completed 42 days of “treatment” at this facility. When I returned home I had a very sour taste in my mouth regrading 12-step programs, however I relied on their belief in “rigorous honesty” and thought if I was honest, everything would work out. So, I called the Pennsylvania board of nursing (BON) and self-reported. I explained that my struggle with problematic substance use began as a way to cope with depression related to divorce (this information is publicly displayed on the boards website): 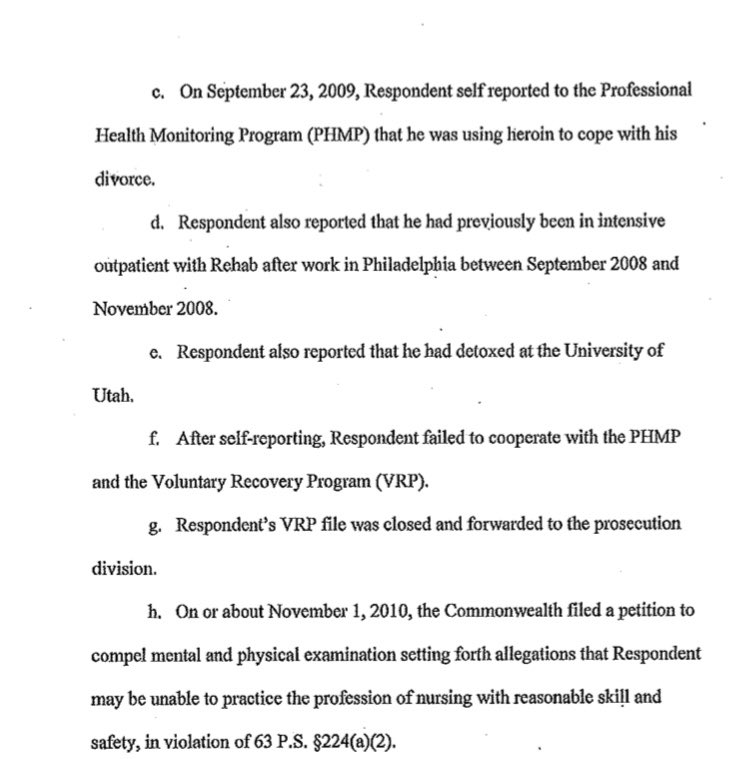 The BON explained that in order to keep my license I would need to agree to entering their program, then called the voluntary recovery program (VRP). The program consisted of more in depth “treatment” including IOP, counseling etc. and 90 12-step meetings in 90 days followed by 3 meetings a week for a period of 3 years, as well as active participation with a sponsor. At this point in my early recovery, and after my experience at Cirque Lodge, I refused to participate in 12-step meetings, and argued that they were a violation of my personal religious rights. The board had a hearing (that I was not notified of) and indefinitely suspended my license. This was in September 2009. I became severely depressed over losing my license and felt like I would never be able to care for sick people again, the career I loved and the one thing that made me feel like my life had purpose. Eventually, I started using heroin again and spent the next two and a half years in active addiction experiencing homelessness. I was eventually arrested for forging a check and spent 6 months in the county jail where I was raped. The BON has a letter I wrote to them on their website (Page 1 Page 2) that is a clear example of how broken I was, but also shows how much I loved being a nurse. It is despicable that this document is posted publicly on their site. When I was discharged I ended up in a Christian recovery program in Philadelphia. Over the next six month period I became interested in the faith and converted to Christianity. I devoted my life to the church and enrolled in bible college. I received a bachelors degree in biblical studies and enrolled in graduate school at Westminster Theological Seminary, where I was studying for the pastorate. During this time I was working for a small community church in Philadelphia’s Kensington neighborhood in their addiction ministry; this is where I met my current wife and got remarried. As a newly married man, I still missed being a nurse and wanted to try to get my license back again, so I called the board of nursing again to try to enroll in the monitoring program, this was in 2012. The VRP had been replaced by the Pennsylvania Peer Nurse Assistance Program (PNAP), however the rules were still the same regarding 12-step programs. At the time I was leading at least 5, but sometimes 8, recovery meetings a week through the addiction ministry, so I asked PNAP if I could substitute those meetings for the 12-step meetings since it would be extraordinarily difficult to fit them in with working full time and being a full time student. PNAP refused to allow me to use faith-based meetings instead of 12-step meetings and, again, held a hearing that I was not aware of and this time labeled me “non-compliant” and placed a mandatory 5 year minimum suspension on my license. I was in recovery for 18 months when I called and had documentation of treatment completion through a 9 month intensive outpatient program, a 12 month residential program, and 18 months of urine drug screens. PNAP would not accept any of the drug screens or treatment, they said I would need to have an assessment done by one of their “approved” assessment centers, begin providing urine drug screens through their contracted laboratory, and follow their guidelines As I continued my theological studies in seminary, my wife and I became foster parents to a 2 week old boy and 4 months later became pregnant with twins. Over the 9 months she was pregnant I became very attached to Micah, our foster son, and I was experiencing growing anxiety that I would lose him some day, as it was looking like he would be reunified with his biological father. When the twins were born, I experienced severe attachment issues stemming from the year long anxiety I felt over potentially losing Micah. This led to a recurrence of drug use, however this was in late 2015, the age of fentanyl. My use escalated quickly and I had a hard time grasping what was wrong. The opioids did not last as long, I was using more times a day than before, overdosing more frequently, and it was much harder to stop than it was 5 years prior. I began going into treatment centers one month into using. Over the next year and a half I entered treatment 16 times. Every treatment center was 12-step, abstinence only based programming. I desperately wanted to re-gain my nursing license and I kept pursuing abstinence because I knew buprenorphine was prohibited by the BON. Many times after I would get out of treatment I would overdose in my home due to reduced tolerance. I would’ve been the perfect candidate for buprenorphine, however I wanted to be a nurse so badly I was prepared to white knuckle recovery, hoping for “the miracle to happen” as they say in 12-step meetings. I eventually abandoned my Christian faith after the church turned their back on me and I found recovery after my 16th time in rehab through the use of Vivitrol (extended release naltrexone). I phoned PNAP and asked to enter the program. At first my case manager said it may only be 90 days until I would be issued a provisionary license. However, that turned out to be an error and she explained that I would need three years of continuous sobriety before I could petition to have my license reinstated. PNAP would monitor me through daily check-ins for random urine drug screens, AA attendance is verified through GPS monitoring on my smart phone, and I had to complete one full year of outpatient addiction treatment.  Over the past 30 months I have participated in three 12-step meetings a week and random urine drug screens. I have consistently noted on monthly progress reports how difficult I find 12-step meetings. I disagree with the spiritual roots of their view of addiction. Having survived a very traumatic relationship with the church I saw very clear parallels between AA and Christianity that were very difficult for me to get through. The meetings made it very difficult to restore my marriage and build relationships with my young children. Most importantly, 12-step fellowships are self-selecting, as is any support group, mandating attendance and participation is counter-productive. Everything we know about recovery tells us that the individual does best when they design their own recovery pathway for themselves. I have made this very clear on my progress reports with the hope that my case managers would understand and realize that 12-step recovery is not a good fit for me. However, the only communication I ever received was a voice mail on July 30, 2019. Listen to the voice mail here. When I called back it was clear that the purpose of her contacting me was to intimidate me into continuing with the meetings. In a subsequent email she stated, “I am sorry the 12-step meetings aren’t working for you…yet” implying a common 12-step philosophy that if you go often enough the program will eventually work for you. Instead of realizing the program wasn’t for me, they continued to mandate me to attend and participate. Over the phone my case manager even told me checking off the box “I go because I am required to” on my monthly progress report form was a red flag to PNAP, which is why she called me. They purposefully created a participation level check box with one box stating the above in order to target who they felt was on the verge of relapse. This further highlights the stronghold the 12-step pathway has in the health professional monitoring program. They view a participant not wanting to go to meetings as a precursor to relapse. 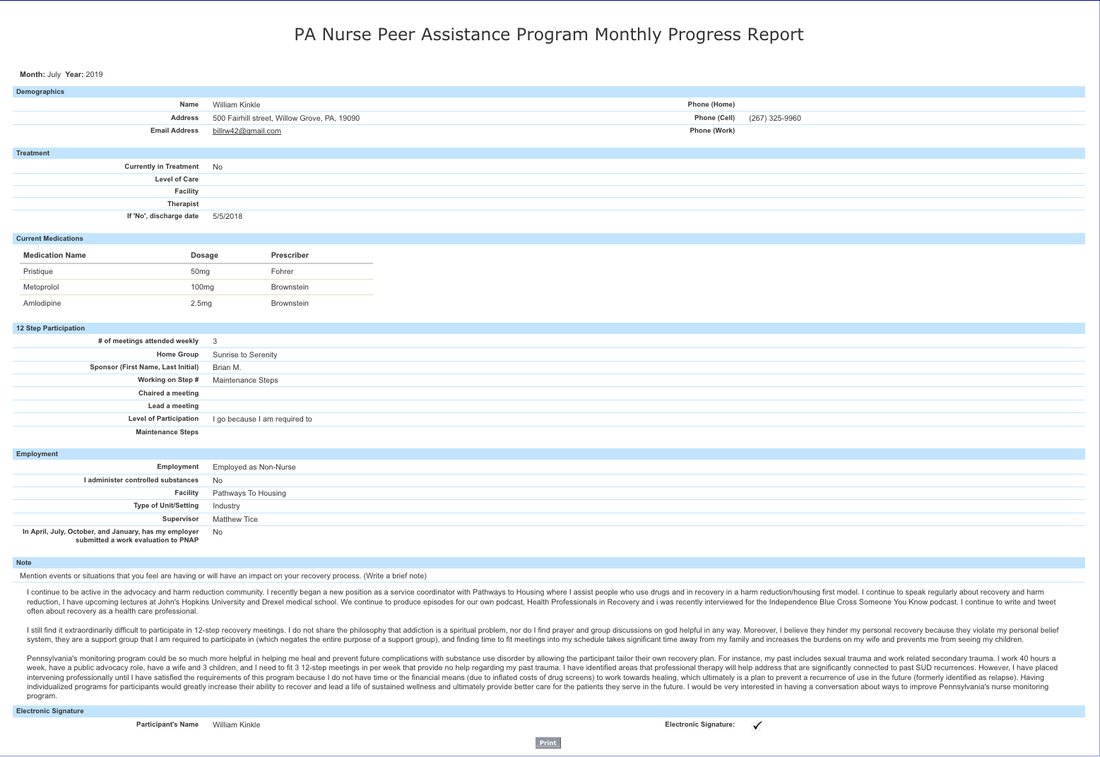 I also describe in detail on every progress report how difficult the procedure is for witnessed drug screens. Every time I am selected for a screen I re-experience being raped. My case manager, a licensed professional counselor, wrote the following email to me: 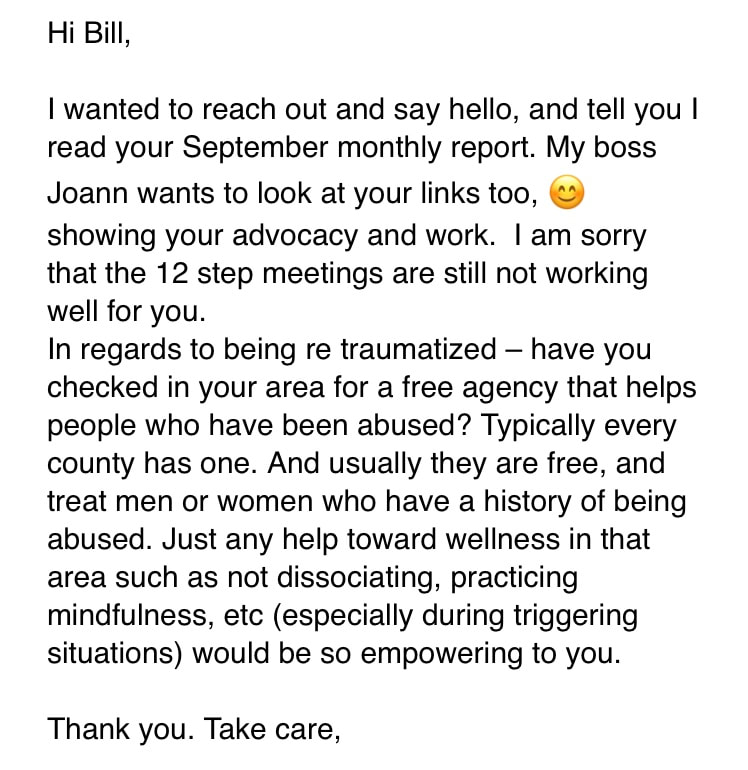 Here was my response to her, which she never answered: 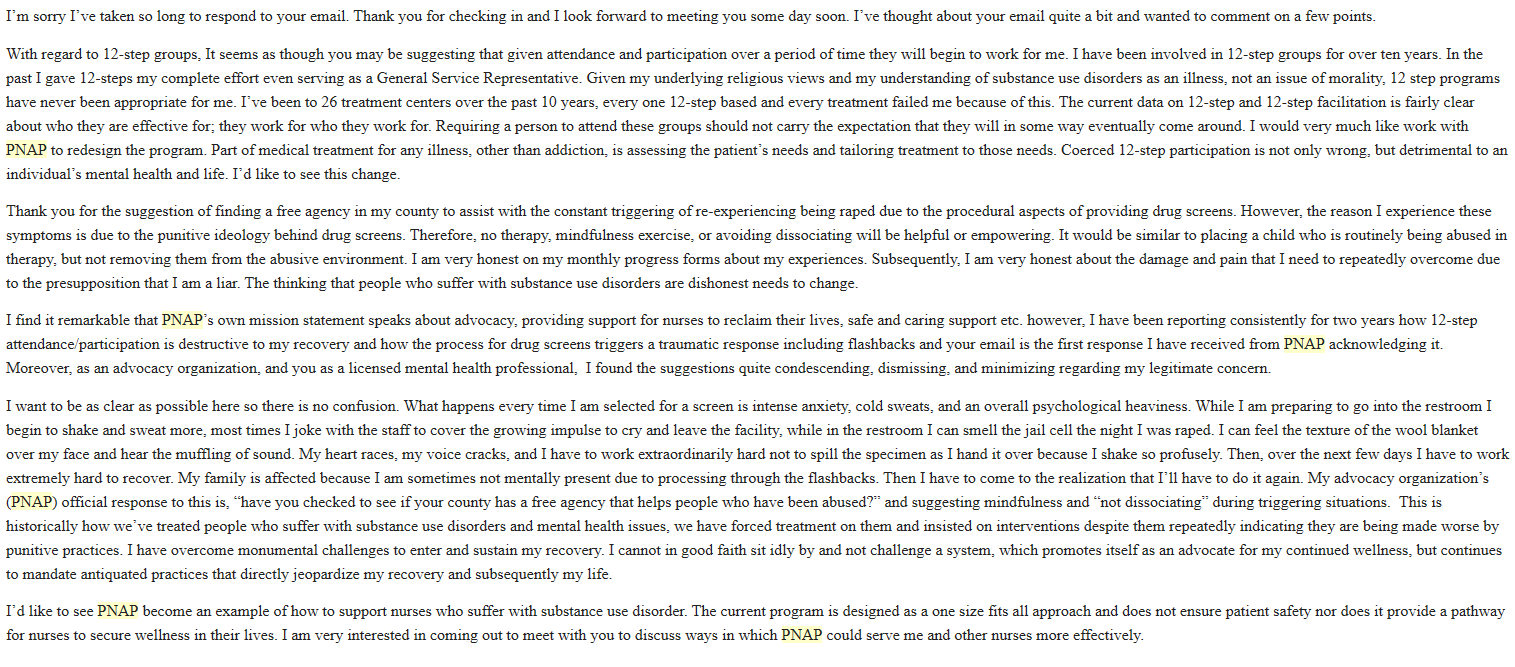 I’ve found it remarkable that a licensed professional counselor, who is my case manager, could ignore a letter explaining what I go through on every screen and not comment on it or offer some form of support. But this has been my experience the entire time I have been a part of this program. PNAP prides themselves to be advocates, however I’ve never experienced advocacy or support through them. From their website: "To identify, intervene upon, advocate for, monitor, and provide support, help, and hope to the Nurse or Nursing Student experiencing Substance Use Disorders, Mental Health Disorders, and/or Physical Disorders that may affect their ability to practice." After 30 months in the program I recently decided to begin taking buprenorphine and I explained my decision-making process in my prior blog post. I emailed my case manager on 4.2.20 to let them know I would be starting opioid agonist therapy and I petitioned to have my license reinstated due to my solid recovery and the current need for nurses due to the coronavirus pandemic. This request was quickly denied, but what struck me was they indicated I was required to provide 5 years of documented recovery, not 3 like I had initially been told. I was under the impression that I had 6 months left until I would be finished with the program. I inquired about the discrepancy and how it was possible PNAP didn't know about the order, this was the email I received: 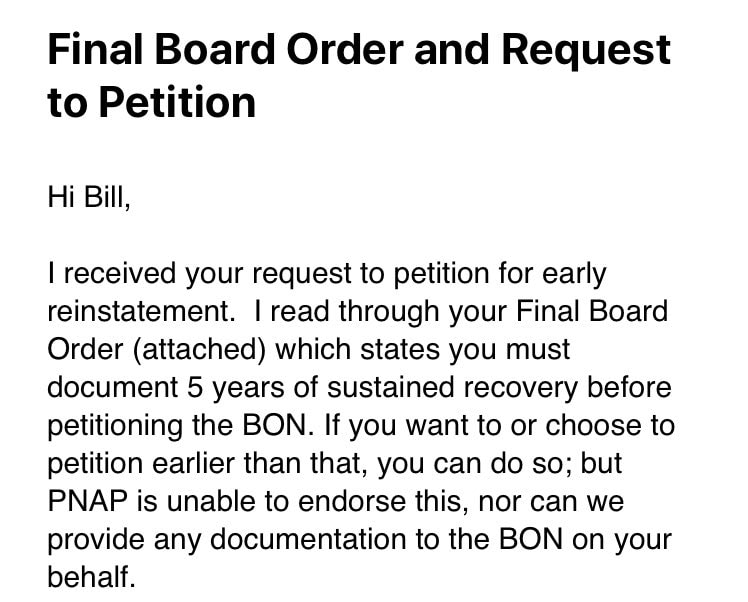 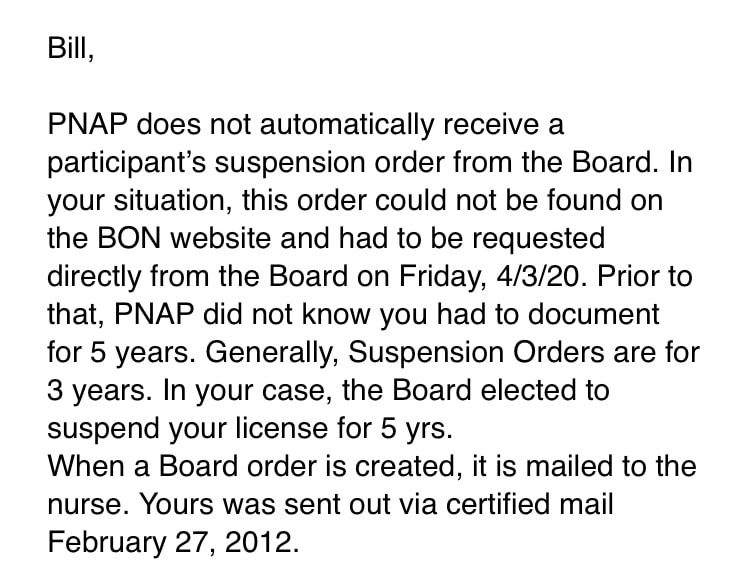 Here is the new board order referenced in the above email that no one has ever seen before: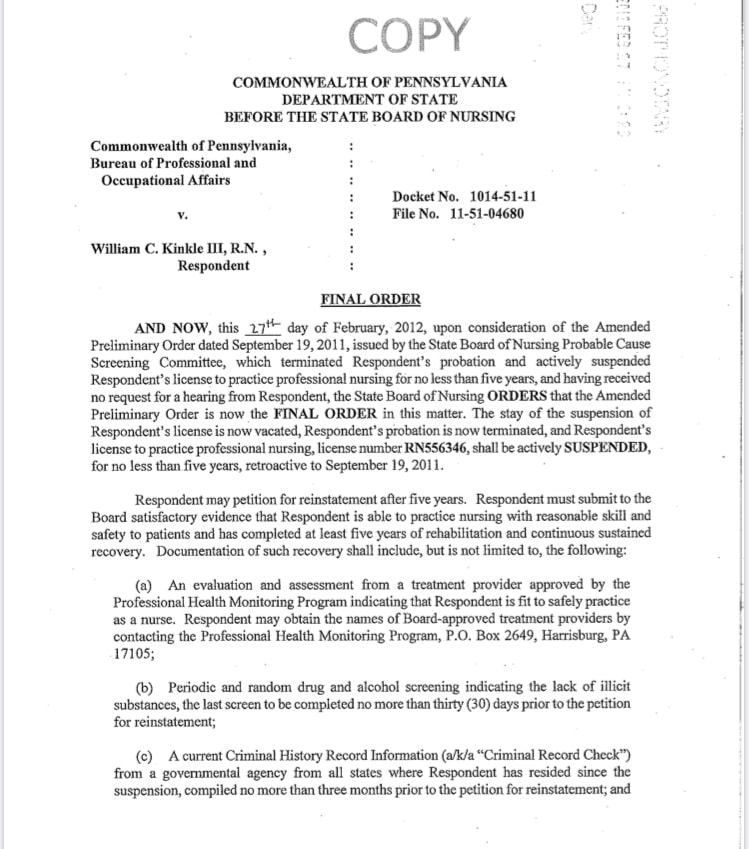 How is it possible that my contract was designed based on a board order from 2012, that they never saw until 4.2.20, and isn’t available on the board’s website for some reason? How is this possible?
Even more interesting, 3 days later I emailed my prescription for my file and PNAP’s response was as if they had no idea I decided to begin taking buprenorphine. It turns out they made the decision to deny my petition for reinstatement without reading my letter. They never had any intention of considering my case. Ultimately what they decided was this, if I will agree to take buprenorphine for a limited time (less than 6 months) they will allow me to stay in the program. However, if I plan on staying on the medication indefinitely, then I will be discharged from the program and my case will be closed. PNAP is forcing me to choose between taking a medication that very well could save my life or continuing to white knuckle through the program and get my license back, so long as I survive, that is. I should also note that I’ve had conversations with PNAP representatives before about OAT and their position on medications for opioid use disorder is, “everyone who uses Suboxone abuses it and are only using it to get high.” There is no question this is a misguided and discriminatory view of OAT. The problem is there are countless nurses out there who have had to decide between their recovery and their career. They have been driven out of the workplace because of an ignorant and antiquated view of medications. Moreover, they have prevented nurses in recovery from practicing. One thing that quickly builds a relationship with a person suffering with a substance use disorder is the comradery gained from having shared lived experience. This opportunity for nurses to bond with a specific patient population is destroyed when you prevent nurses in recovery, and nurses who have taken a pathway to recovery through the use of medications, from entering the clinical space. This is where I stand right now. I must decide between my own recovery, safety, and wellness or pursuing the career I loved in order to care for the patients I love. What a crappy place to be. Some noteworthy points for discussion. My PNAP contract states any biological specimen provided from me becomes property of the commonwealth and they will not release results or records to anyone under any circumstances. This means if I had a screen that yielded a positive result, I would not have a right to see the result. Moreover, now that I am being discharged from the program I cannot have any of my supporting documents to petition the BON directly. 30 months of negative screens, assessments, treatment records, and AA attendance logs are all their property. The financial aspect of being in the program resulted in my wife and I having to declare bankruptcy due to the piling up of debt. There are annual supervision fees associated with being in the program. Every time a participant is selected for a screen there is a fee that goes to the lab for analysis and there is an arbitrary fee paid to the collection site. Collection sites can choose to charge whatever they want for collecting the urine and mailing it to the lab. Fees range from $20-80. Interestingly, at one collection site a urine sample costs $30, however if it was a blood sample they charge $10. I inquired why, understanding that collecting a blood specimen utilizes more materials and should therefore be more expensive. The collection site explained that they charge inflated fees for urine because it is the most common sample form, therefore they can make more money. There is a major conflict of interest regarding the mandatory assessments required by the BON. Assessments must be completed by “approved” centers. However, these assessment sites are usually through large treatment facility chains. Whatever the assessment recommendations are, the participant must complete according to their PNAP contract. Therefore, there is financial gain to be made by the assessor recommending the maximum and most invasive treatment path. I have thought considerably about the past 12 years of my life. I’ve often wondered how things may have been different if there was a culture in health care that normalized professionals struggling with substance use disorders. I would have been more likely to ask for help before I ended up homeless and in jail. If 12-step recovery wasn’t the only exclusive option, perhaps I would’ve entered the program earlier. Had I been in the program and practicing as a nurse in 2015 I may have had an entire support network to assist me manage all the issues surrounding Micah’s adoption. I may have never suffered a recurrence of use. I also think of the hundreds of patients who I could’ve met as a nurse who are struggling themselves. How powerful would it have been to disclose that I have been through what they were experiencing. How many lives could’ve been saved if we would only develop a system that truly offers peer support and allows the individual to exercise autonomy over their own recovery pathway; a recovery plan tailored and designed for them and their unique needs. These are big questions that I don’t know the answer to. However, I do know that everything must change. How we treat our own as healthcare professionals is deplorable, despicable, and is an eye sore for our respective professions. I cannot let it continue. You can access my Pennsylvania Board of Nursing records here: https://www.pals.pa.gov/#/page/searchresult
2 Comments
4/7/2020 6 Comments Why I Decided to Start Taking Buprenorphine After Being Abstinent for Two and a Half Years Living in a culture that views abstinence as the ultimate goal when thinking about recovery it may seem quite difficult to understand why a person might decide to begin opioid agonist therapy (OAT) after a long period of abstinence. I’m sure I’ll get a lot of questions from folks trying to understand my decision. In the same way, I am also certain I’ll receive quite a bit of support for this decision. My hope in writing this is to help you understand my decision-making process and what I hope to get out of taking buprenorphine.
I’ve written and spoken about the role of vicarious, or secondary, trauma and its relationship to my personal struggle with substance use, primarily heroin (opioids). Over the years as I’ve thought critically about how drugs became a part of my life at 34 years old it became clear that something predisposed me to finding solitude in drug use. One factor that played a part in driving my use was being in a profession that placed me in a world of pain. As a paramedic and as a nurse I knew that every day I would spend my time interacting with people who were suffering, and my job was to alleviate their pain to the best of my ability. For some reason, I have never been the type of person who could “leave it at work.” I’ve often been described as an “empath” by others, largely because I have always found it difficult to find the dividing line between the pain of the world and my own personal pain. The medical professions (nurses, physicians, paramedics etc.) are very stoic and embrace a culture of mental toughness. This culture has some benefits, however when one of our own begins to suffer it creates an environment that leaves little room to ask for help. Particularly when the individual is suffering with something as heavily stigmatized as drug use, this was my experience. When I began to suffer with problematic substance use, I felt a deep shame that prohibited asking for assistance. Moreover, I worked in an emergency department and I saw how people suffering with addiction were treated, because of this it was impossible for me to ask my peers for help and I suffered in silence. The years of compounding secondary trauma I experienced caring for critically ill people, along with the helplessness I felt when I couldn’t help someone due to severity of illness, or the many systemic barriers which made it difficult to properly care for someone, had a profound effect on me. I was unaware of the toll it took, and how much it chipped away at me over the years. However, what it did was set up a vulnerability so under the right circumstances I could develop what is described as a “substance use disorder,” for me, those conditions were depression. I’ve encountered severe, uncontrolled drug use twice in my lifetime and both times were directly related to severe depression. Using drugs, primarily opioids, was an attempt to anesthetize the pain from mental illness. Both times were triggered by high level stress events, the first divorce and the second was the fear of losing a child. Over the years I’ve been able to dissect these events and develop plans to mitigate the effects of stress in order to prevent a recurrence of drug use. However, there is little I can do regarding the pain around me. “Self-care” is somewhat of a buzz word that is casually thrown around as the cure all for preventative medicine. However, I’ve never been able to figure out what self-care looks like in the practical sense. Particularly when my life is devoted to helping people who have been marginalized by society. I currently work in the drug user community in Philadelphia. I have a reputation with this group as someone who understands the struggle because I’ve been through it. When introducing me to new people folks often begin with, “Bill is one of us.” It’s the only time I am honored to be called a “junkie” or a “drug addict,” because their intention by using those words is endearment, not a negative connotation. My experience and understanding of drug use carry significant weight to them. However, with this honor comes trust and through this trust I have the privilege of hearing their deepest and darkest secrets. I often witness some of the most horrific trauma and pain imaginable. As I’ve explained, I sometimes have a difficult time finding the dividing line between their pain and my own, this takes a toll. I cannot imagine doing another job. I love what I do. This job gives my life significant meaning and purpose. I can’t think of anything I would rather do than help my comrades still in the trenches. My recovery is solidified in the work of helping others. Although I am sometimes critical of 12-step fellowships, this is one area I very much respect, helping those still suffering. Even though this job gives my life purpose and satisfaction, there is a risk for me that comes with living in a world filled with so much pain. Particularly, during the COVID19 pandemic. Therefore, I’ve decided to start taking buprenorphine. I’ve added it as a safety net in a sense. I’ve listened to others who are in recovery through medications like methadone and buprenorphine who often discuss abstinence as "white knuckling it" through recovery. It helped me realize that there have been times over the past two and a half years where I have unnecessarily suffered through urges to use in an effort to “soften the blow” of vicarious pain. Although these urges are transient and I am able to work through them, I am not convinced I need to do so just to prove I can do abstinence. I am particularly concerned that there may be a time in the future, as stress and uncertainty increase, where I may make a rash decision under the right circumstances and use opioids. Especially because I work in an area where they are available on every street corner. The drug supply in Kensington, Philadelphia is grossly contaminated and poisoned, which means a split-second decision to use could very well end my life. Buprenorphine is a sound decision to reduce that risk. I need to make a clear distinction here with regards to people, places, and things (PPT). PPT is a mantra we are often taught in treatment centers and 12-step programs indicating you must change everything about your old habits and refrain from being around anything that you relate to drug use. Me being in Kensington, visiting my friends up on the railroad tracks in their encampment where they are all actively using would be considered an activity I should avoid due to triggers. However, I need to make a distinction here. Being around drugs, or people using drugs, does not generate cravings in my mind. After two years of being around it I am fairly desensitized. What I am describing is a deeper level of understanding about myself and what drove my use initially back in 2008. I believe this is the wisdom that comes from solid introspective recovery work. I’ve begun to develop a working knowledge of what makes me tick and from this knowledge I’ve been able to develop a safety plan. The decision to begin taking buprenorphine was birthed out of this work and is a way to continue to strengthen my recovery. Starting OAT after 2.5 years of abstinence doesn’t weaken my recovery, it is a well thought out and wise decision to further secure my recovery. Life isn’t stagnant, we often experience changing parameters and we must adjust to the changes around us. My life has changed, the emotional demands on me have changed. Therefore, the safeguards I need to have in place need to change. I should also note that I didn’t make this decision unilaterally. I spoke with several people I trust and respect, including an addiction medicine physician to ask for their counsel after fully disclosing the reasons I’ve outlined here. In addition to the above reason, I also feel I will be a better advocate for the patients I care for. There is quite a bit of self-stigma present in the community regarding buprenorphine. Me being able to share my transition to the use of medications to bolster my recovery will provide a safe environment for people to ask questions and not feel judged. I also think having a long period of abstinence before medication also challenges the paradigm a lot of us have always thought about medications for opioid use disorder. I’ve also written about health professional monitoring programs and their unofficial prohibition of OAT. Initiating OAT after 30 months of abstinence will provide me an opportunity to experience first-hand what happens “officially” because I am a participant in one of those programs. Overall, I believe this is the next step in my recovery journey. I don’t have a timeline for tapering off. I am interested to see if buprenorphine will reduce the “noise in my head” that gets overwhelming at times. I figure it’s worth the effort to try, if it doesn’t help, I can always go back to abstinence. This is a very low risk endeavor. I recently posted on social media, "Drugs don't make people lie, steal, or manipulate. We Do" and attached the hashtags #shame #stigma #prohibition #criminialization I received a fair amount of pushback. Mainly, it was people recalling their own behavior while in active addiction, but they didn't detail why they did those things. I think the answer lies in investigating this question, the "why" do we lie, steal, and manipulate. Below is a response I posted to someone asking for an explanation.
It's easy to look at different behaviors that we commonly associate with people who struggle with problematic substance use like lying, stealing, manipulating, etc. and say they are a result of using drugs. However, we need to look deeper if we care about helping people. We have to ask the questions, why do people lie? Why do people steal? Why do people manipulate? It’s easy to blame it on the drugs. One reason it’s easier to do this is it absolves us of any responsibility to invest the time and energy it takes to understand the issues and it gives us a pass to challenge laws and policy that foster those behaviors that repulse us, it feeds the notion that addiction is about morality and poor decision making. Most people who struggle with addiction lie because they feel like no one will understand the reason they use. Most people will not be able to comprehend the monumental pain they live with without the drug. Moreover, most of us have learned from past experience that honesty usually results in a negative or punitive response from others; or folks start to tell us what they think we “need” to do, which isn’t helpful. So we lie to avoid being spoken down to or having our pain minimized. Another reason is the shame that comes from drug use. Our society has a long romance with villainizing people who use drugs through policy and media. Most reality shows, TV, and film portray drug use as a deviant criminal exercise, this subconsciously impacts and persuades us to look at folks who use certain substances differently than we do others. This further affects how we speak to and deal with our friends and family who use certain drugs. Moreover, if you study American drug policy history you will find that discrimination is at the heart. Our drug policies weren’t created to make people healthier or improve families, well at least not SOME families. Drug policy is all about racism and xenophobia and this has come to be extended to poor whites as well to some extent. We have to look at the origins of our laws and how they have been exploited to shape our beliefs about certain subsets of the population. Read about: Harry Anslinger The Harrison Act of 1914 The Volstead Act of 1919 The Federal Bureau of Narcotics in 1930 The Marijuana Tax Act of 1937 The Comprehensive Drug Abuse Prevention and Control Act of 1970 The difference between our nations response to crack cocaine vs opioids If you learn about his history you’ll start to see some stunning patterns that shape how we feel about certain drugs and the people who use them today. By prohibiting certain substances and criminalizing their possession and use we have created a sub-class of people that most of the country views negatively. This dramatically affects how we see them and how we interact with them. Most of our interactions and judgments are out of fear and ignorance. We think we know why they are doing what they are doing, but we really don’t. Most of our understanding comes from TV and what we hear from others. If certain substances were legal, regulated, and dispensed for people who needed them, stealing, manipulating and lying would go away. Most people who use illicit substances procure them illegally, therefore getting and using them comes with inherent risk of arrest and other consequences. When people habitually use certain substances there is a brain chemistry component that is helpful to understand as well, particularly when thinking about the lying, stealing issue. Over time drug use becomes tied to a very primitive part of the brain. It is viewed on the level of necessary for survival, similar to food, shelter, breathing etc. This occurs on a subconscious level, but it drives behavior. Therefore, when a person is without the needed substance their brain views it as a crisis and something that must be procured for survival. Imagine one day food becomes illegal and scarce. What lengths would you go to in order to secure food for yourself and your family? What laws would you break and what lies would you tell to get what you need? This is how it is for the person who uses drugs after a period of time. Now imagine if eating food was highly stigmatized and most of society has portrayed food eaters as low life, scum bag, liars, cheaters and thieves? How likely would you be to openly discuss your desire and need for food with another? You’d feel pretty ashamed and go to extreme lengths to hide it, right? It’s not a perfect analogy, but I hope my point is taken. The bottom line is this, just because a person takes a drug doesn’t automatically mean that person will lie, steal, or manipulate. The factors that drive these behaviors have to do with societal and social expectations and influences. If we aim to help our drug using friends, we need to be willing to look at the myriad of other issues that drive those behaviors that repulse us so much. Otherwise we will only be pushing our expectations on them and never really help them. Case in point. I meet with people who actively use daily. Many of them are looking for help with stopping or moderating use to mitigate negative consequences. These folks know I won’t ever judge them for using and we talk openly about goals, set backs, and ways forward. There is no expectation on my part that they will stay abstinent. Therefore, shame is removed from use. They know they don’t need to impress me with doing what they think I want them to do. Because of the focus being on them and their lives, instead of outside goals and expectations they are exceptionally honest. They are honest because they know there will be no judgement with me and because they know all I care about is helping them be happy and content with their lives. Essentially, I treat people how I wish someone treated me when I was struggling. Really it’s how every human being wants to be treated, with kindness, compassion, and understanding. 1/6/2020 0 Comments How I got into RecoveryMany people have asked what helped with my recovery. Here are more details outlining what was helpful for me. It’s important not to take this as a template for anyone else. What I did was specifically tailored to me given the complexity of my life and the independent work I did to learn what was important to me.
When I relapsed I was in a second career because my nursing license was indefinitely suspended. I was working in Christian ministry as a pastoral intern for a homeless and addiction ministry and I was a second year graduate student in seminary. I had strong religious convictions and as a result viewed addiction as an issue of sin/morality. Over the 2 year period I was injecting opioids (heroin and fentanyl) I immersed myself in church, prayer, and seeking guidance from spiritual leaders in the church. Over time I realized that no one knew what to do when their star student at a prestigious seminary said, “I can’t stop shooting heroin and I don’t know what to do.” Ultimately, they did nothing. Trish and I went to 4 different churches and begged for help, we were outcast from the fellowship because I was in “rebellion against god and living in sin.” We were foster parents of a 1 year old and had newborn twins at the time. Over the 2 years we worked closely with the foster care social worker (who was in recovery) and as long as we were trying to get in recovery she supported us. As soon as I realized I was dependent and addicted I started seeking help. I desperately wanted to be in recovery, however this was the second time I fell into deep addiction and it was during the current fentanyl era. I found it extraordinarily difficult to stop, much harder than the first time. I was using 4-6 times a day, getting sick more often, and overdosing with frequency and I couldn’t figure out why. I knew I wanted to be a nurse again and for this to happen I could not be on buprenorphine or methadone. I had to choose a path of abstinence. At the time I also believed those medications were just trading one drug for another and I’d still be “sinning” based on my religious convictions and theological underpinnings. Over an 18 month period I went into inpatient treatment 16 times. I started using within 3 hours of discharge on 15 of those 16 admissions. After #14 I decided I would try naltrexone to “self detox,” so I locked myself in a hotel room with 2 trusted friends, used 20 bags of heroin and took a 50mg naltrexone tablet. I spent 3 days experiencing vomiting, intense diarrhea and hallucinations. As soon as I was lucid I left and used again. It was a horrible experience. After about 2 more weeks of using we found an addiction medicine physician who I convinced to administer the Vivitrol injection. I lied and said I had been absintent, primarily because I was so desperate and wanted to be in recovery so badly I was willing to do anything. However, after 1 day of intense withdrawal I resumed using 4 times a day and continued to for over a month. I mixed injecting with benzodiazepines to try to buffer the symptoms. Over this time period and after 2 years of being abandoned by the church I was spending a considerable amount of time trying to understand and figure out what I believed about god. I questioned all of the theology that undergirded my life at that point. So much of it was wonderful in theory, but practically it was useless and destructive. So, I decided to abandon my faith. I went to see my addiction doc and told her I was continuing to use and she strongly recommended inpatient treatment. I was terrified to go away for a 16th time. Trish was at the breaking point, our marriage was becoming unstable, the kids were exhibiting signs of being taxed by daddy always going in the hospital, and financially we were bankrupt from drug money, insurance premiums, co-pays, me not working, and doctor visits. All three of us had a deep conversation and I went into treatment for the 16th time in 18 months. When I called admissions the coordinator refused to let me come in. She said I’ve been there too may times and clearly don’t want to do the work. I remember my heart sinking and strongly considering suicide. I wasn’t sure what to do. I couldn’t stop using, I’m so bad that the treatment centers won’t even let me in, I was putting my family at risk of losing our son, and I couldn’t live with the shell of the woman Trish had become because of my addiction. But then Trish sent me a text saying, “you need to get it together and get better. You are the most tenacious man I have ever met. Please get help.” Her support alleviated all of the worthlessness I felt long enough for me to feel empowered to do something. I drove to the treatment center and told them I refused to leave until they agree to admit me. The CEO eventually came down and met with me and they agreed to admit me as long as I agreed to a special program for habitual offenders. So that’s what I did. Given my recent thread about treatment centers you might be curious why I’d subject myself to the same experience. First, my thoughts about treatment are retrospective after several years of critically thinking about what went wrong and looking at treatment through a different lens. When I went in I was desperate and suicidal. Second, the staff at this treatment center were genuine, kind, and compassionate. They met me at the door with a smile and said they were happy to see me again. They carried my bags when I was in withdrawal. They sat with me all night long when insomnia was at its peak talking about life. The humanity they displayed was something I needed and it played a huge part in saving my life. The staff I am identifying here are the techs. They are peers in recovery who make the centers run. They are the ones you spend most of the time with. They run most of the groups. They made an unbearable situation bearable. I committed to 1 year of investing myself into a 12-step program. I decided to abandon Christianity and try AA. It was very difficult for me to grasp the spiritual aspect of the program given the trauma I experienced with the church. There were too many parallels between AA and Christianity and my disconnection from the church was too proximal. Remember, I recently finished a bachelors degree in bible and was a second year seminary student; meticulously dissecting theological beliefs was the norm for me. One of AAs strong points is its belief requirements are incredibly malleable in order to be applicable to the widest audience. However, for someone like me who came from a staunch, confessional, reformed, Presbyterian background the looseness of AA was almost impossible for me to comprehend practically. Ultimately, working a 12-step program is what solidified my atheism. I spent the first year listening to AA beyond belief and finding great comfort there, but ultimately the amount of effort I needed to exert in order to circumvent the religious aspects of the 12 steps were counterproductive; so I created my own recovery support network, which largely came from the Twitter community. After discharge I had employment immediately and I enrolled in my state’s nurse monitoring program. Now, I need to be very clear about the role of the nursing program. What gives me the drive to sustain my recovery aren't the programmatic aspects; rather, it’s the hope that I’ll be able to be a nurse again. Nothing that I do as part of the monitoring program supports my recovery. In fact, it threatens my sustained recovery. I write about this often. I am mandated to 3 12 step meetings a week and required to actively participate in the program,. In addition, the procedural aspects of random drug screens are dehumanizing and traumatic because I am a rape survivor. I have expressed this in writing 27 times via monthly progress reports to my case manager and the only responses I’ve received are, “sorry AA isn’t working for you yet” and “try to take some steps toward wellness (re: abuse history) and when you’re in triggering situations try not to dissociate and practicing mindfulness would be empowering to you.” What keeps me in recovery is looking forward to being a nurse, not the threat of consequences from drug screens and certainly not being mandated to 12 step meetings. This is important. Also worth noting that I have identified several areas in my life that increased my vulnerability to developing an opioid use disorder and trauma is the main common denominator. Past sexual trauma and vicarious trauma acquired from 15 years working in intense emergency medicine environment took its toll. I find it disgustingly fascinating that part of my recovery plan is to regularly re-traumatize myself by placing me in an environment where I predictably experience flashbacks. The exact reasons I used drugs in the first place were to suppress the feelings I now am mandated to re-experience in order to prove I am "sober." The most important thing that got me in recovery are my family. My wife who was essentially a stay at home mom for 3 toddlers while I was away in treatment. She paid the bills, my insurance premiums, co-pays, managed the house, worked full time as a social worker in the child welfare system, interacted with our son's social worker and adoption agency, and loved on me infinitely. They are the reason we recovered and the driving force behind why we stay recovered. Other things worth mentioning: Just because I had some positive interactions in treatment doesn’t mean treatment was necessary or worked. As I’ve outlined, there were many other things at play outside of treatment. If I was not white I wouldn’t be in recovery and I would’ve lost my son. The privilege I benefited from by being white needs to be acknowledged. The basic fact that I entered treatment 16 times in 18 months defines privilege. We need to talk about this. Another key ingredient for me was advocacy. I watched ‘The Anonymous People” documentary after my last inpatient stay and it had a profound impact on me. It gave me the green light to be public about my recovery. Being transparent and open has empowered me in ways I’ve never dreamed were possible. I went from living in shame, trying to hide aspects of my life to being in control of my story and empowered. I’m grateful for the recovery movement pioneers. Being a paramedic and a nurse in recovery has its own unique subtleties. Healthcare professionals rarely speak openly about their struggle with addiction and, more importantly, their recovery. This is why we started the Health Professionals in Recovery podcast and why I am committed to pushing for a recovery movement in medicine. We need it for ourselves and our patients. What sustains my recovery is having a drive and purpose in life. I am always working towards goals, fabricating ways to accomplish those goals, and my goals are designed to make the world a better place in some small way. Recovery is about purpose and passion. Until I figured out what I wanted my life to be about, there was no hope of stopping drug use. Now that I have purpose, direction, passion, and support, I don’t need or desire drugs. But that’s just me. |

Bill Kinkle
Bill is a paramedic and nurse in recovery from opioid use disorder who cares about dispelling common myths about people who use drugs, addiction, and recovery. ArchivesCategories |
 RSS Feed
RSS Feed

{kind=link}
{kind=link}