|
4/7/2020 6 Comments Why I Decided to Start Taking Buprenorphine After Being Abstinent for Two and a Half Years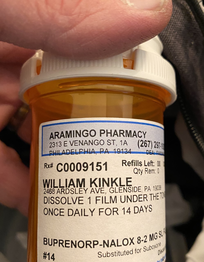 Living in a culture that views abstinence as the ultimate goal when thinking about recovery it may seem quite difficult to understand why a person might decide to begin opioid agonist therapy (OAT) after a long period of abstinence. I’m sure I’ll get a lot of questions from folks trying to understand my decision. In the same way, I am also certain I’ll receive quite a bit of support for this decision. My hope in writing this is to help you understand my decision-making process and what I hope to get out of taking buprenorphine.
I’ve written and spoken about the role of vicarious, or secondary, trauma and its relationship to my personal struggle with substance use, primarily heroin (opioids). Over the years as I’ve thought critically about how drugs became a part of my life at 34 years old it became clear that something predisposed me to finding solitude in drug use. One factor that played a part in driving my use was being in a profession that placed me in a world of pain. As a paramedic and as a nurse I knew that every day I would spend my time interacting with people who were suffering, and my job was to alleviate their pain to the best of my ability. For some reason, I have never been the type of person who could “leave it at work.” I’ve often been described as an “empath” by others, largely because I have always found it difficult to find the dividing line between the pain of the world and my own personal pain. The medical professions (nurses, physicians, paramedics etc.) are very stoic and embrace a culture of mental toughness. This culture has some benefits, however when one of our own begins to suffer it creates an environment that leaves little room to ask for help. Particularly when the individual is suffering with something as heavily stigmatized as drug use, this was my experience. When I began to suffer with problematic substance use, I felt a deep shame that prohibited asking for assistance. Moreover, I worked in an emergency department and I saw how people suffering with addiction were treated, because of this it was impossible for me to ask my peers for help and I suffered in silence. The years of compounding secondary trauma I experienced caring for critically ill people, along with the helplessness I felt when I couldn’t help someone due to severity of illness, or the many systemic barriers which made it difficult to properly care for someone, had a profound effect on me. I was unaware of the toll it took, and how much it chipped away at me over the years. However, what it did was set up a vulnerability so under the right circumstances I could develop what is described as a “substance use disorder,” for me, those conditions were depression. I’ve encountered severe, uncontrolled drug use twice in my lifetime and both times were directly related to severe depression. Using drugs, primarily opioids, was an attempt to anesthetize the pain from mental illness. Both times were triggered by high level stress events, the first divorce and the second was the fear of losing a child. Over the years I’ve been able to dissect these events and develop plans to mitigate the effects of stress in order to prevent a recurrence of drug use. However, there is little I can do regarding the pain around me. “Self-care” is somewhat of a buzz word that is casually thrown around as the cure all for preventative medicine. However, I’ve never been able to figure out what self-care looks like in the practical sense. Particularly when my life is devoted to helping people who have been marginalized by society. I currently work in the drug user community in Philadelphia. I have a reputation with this group as someone who understands the struggle because I’ve been through it. When introducing me to new people folks often begin with, “Bill is one of us.” It’s the only time I am honored to be called a “junkie” or a “drug addict,” because their intention by using those words is endearment, not a negative connotation. My experience and understanding of drug use carry significant weight to them. However, with this honor comes trust and through this trust I have the privilege of hearing their deepest and darkest secrets. I often witness some of the most horrific trauma and pain imaginable. As I’ve explained, I sometimes have a difficult time finding the dividing line between their pain and my own, this takes a toll. I cannot imagine doing another job. I love what I do. This job gives my life significant meaning and purpose. I can’t think of anything I would rather do than help my comrades still in the trenches. My recovery is solidified in the work of helping others. Although I am sometimes critical of 12-step fellowships, this is one area I very much respect, helping those still suffering. Even though this job gives my life purpose and satisfaction, there is a risk for me that comes with living in a world filled with so much pain. Particularly, during the COVID19 pandemic. Therefore, I’ve decided to start taking buprenorphine. I’ve added it as a safety net in a sense. I’ve listened to others who are in recovery through medications like methadone and buprenorphine who often discuss abstinence as "white knuckling it" through recovery. It helped me realize that there have been times over the past two and a half years where I have unnecessarily suffered through urges to use in an effort to “soften the blow” of vicarious pain. Although these urges are transient and I am able to work through them, I am not convinced I need to do so just to prove I can do abstinence. I am particularly concerned that there may be a time in the future, as stress and uncertainty increase, where I may make a rash decision under the right circumstances and use opioids. Especially because I work in an area where they are available on every street corner. The drug supply in Kensington, Philadelphia is grossly contaminated and poisoned, which means a split-second decision to use could very well end my life. Buprenorphine is a sound decision to reduce that risk. I need to make a clear distinction here with regards to people, places, and things (PPT). PPT is a mantra we are often taught in treatment centers and 12-step programs indicating you must change everything about your old habits and refrain from being around anything that you relate to drug use. Me being in Kensington, visiting my friends up on the railroad tracks in their encampment where they are all actively using would be considered an activity I should avoid due to triggers. However, I need to make a distinction here. Being around drugs, or people using drugs, does not generate cravings in my mind. After two years of being around it I am fairly desensitized. What I am describing is a deeper level of understanding about myself and what drove my use initially back in 2008. I believe this is the wisdom that comes from solid introspective recovery work. I’ve begun to develop a working knowledge of what makes me tick and from this knowledge I’ve been able to develop a safety plan. The decision to begin taking buprenorphine was birthed out of this work and is a way to continue to strengthen my recovery. Starting OAT after 2.5 years of abstinence doesn’t weaken my recovery, it is a well thought out and wise decision to further secure my recovery. Life isn’t stagnant, we often experience changing parameters and we must adjust to the changes around us. My life has changed, the emotional demands on me have changed. Therefore, the safeguards I need to have in place need to change. I should also note that I didn’t make this decision unilaterally. I spoke with several people I trust and respect, including an addiction medicine physician to ask for their counsel after fully disclosing the reasons I’ve outlined here. In addition to the above reason, I also feel I will be a better advocate for the patients I care for. There is quite a bit of self-stigma present in the community regarding buprenorphine. Me being able to share my transition to the use of medications to bolster my recovery will provide a safe environment for people to ask questions and not feel judged. I also think having a long period of abstinence before medication also challenges the paradigm a lot of us have always thought about medications for opioid use disorder. I’ve also written about health professional monitoring programs and their unofficial prohibition of OAT. Initiating OAT after 30 months of abstinence will provide me an opportunity to experience first-hand what happens “officially” because I am a participant in one of those programs. Overall, I believe this is the next step in my recovery journey. I don’t have a timeline for tapering off. I am interested to see if buprenorphine will reduce the “noise in my head” that gets overwhelming at times. I figure it’s worth the effort to try, if it doesn’t help, I can always go back to abstinence. This is a very low risk endeavor.
6 Comments
Stina Adams
4/7/2020 07:54:57 am
I support you 100%. I understand the trauma of the healthcare field. It only took 2 years to send me into panic attacks and depression. Take care of yourself so you can continue giving back. Sending love and support.
Michelle
4/7/2020 08:37:53 am
Best of luck, and health to you. It is inspiring to see a medical professional living harm reduction practices.
Charlotte Ross
4/7/2020 03:49:00 pm
Wishing you all the best of health in your recovery. I totally support your decision, both on the bases of science and personal choice. 4/7/2020 04:01:18 pm
powerful and compelling Bill; your authenticity and openness in speaking your truth is inspirational for me. I'm sure it is for many folks. Thank you for sharing.
Genna M
4/7/2020 07:36:30 pm
Bill,
Laura
4/8/2020 12:20:32 pm
Bill, just a thank you for sharing your story with such a clear message of the inherent conflicts at play when we say people in recovery are either 'worthy' or 'unworthy'. It's bullshit and you don't deserve to be treated differently because of who you are or what you believe. I hope you keep us all updated and that your recovery continues to progress. Leave a Reply. |

Bill Kinkle
Bill is a paramedic and nurse in recovery from opioid use disorder who cares about dispelling common myths about people who use drugs, addiction, and recovery. ArchivesCategories |
 RSS Feed
RSS Feed
